Torticollis is a condition which affects the neck and spine in many infants. A common name for Torticollis is "wry neck". The literal translation is "crooked neck". It is a very treatable condition, but should be taken seriously and treated by your child's pediatrician.
The first signs of
Torticollis may not appear until the infant is 2-3 months old. You may notice that your child stares into one direction. Your child may seem to hold his neck to the side, and you may even notice a sizable lump just above the infant's collar bone.
The condition affects the sternocleidomastoid muscle which connects the base of the skull to the collar bone. This muscle is the main muscle that is used to move the head from side to side. In an infant with
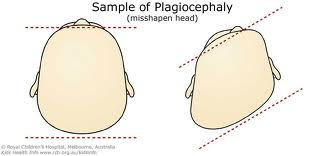
Torticollis, the muscle is shorter on the side that the head is tilted to. With treatment, the muscle will grow and stretch; but if left untreated the condition may cause a permanent limitation of the infant's neck movement. If action is not taken, the infant's head may flatten on one side and the face may become mis-formed.
There are several theories as to what causes
Torticollis in infants, but the main theory is the limitation of space inside the mother's uterus. The infant may be stuck in one position for a period of time and not able to move its neck, which in turn will affect how the muscle is formed. If the infant has had a limited amount of mobility of the neck in the womb, the muscle will be very stiff and tight.
Once diagnosed, you will want to start a serious of stretching exercises with your infant. The most basic stretch consists of laying the infant on his or her back and rotating the head away from the tilt. This will
stretch the sternocleidomastoid muscle and relieve the tightness. One other very simple but extremely affective stretch involves laying the infant on its back and tilting the head gently to the side opposite of the tilt. Be sure to only stretch small amounts so that the muscle does not tear or become stressed. Watch your infant for any signs of discomfort, and never stretch past a comfortable pull. Repeat these exercises several times through out the day to lengthen and loosen the muscle.
It is also important to reposition your child's head. If the infant sleeps with its head turned one way a flat spot may shape on the side of the skull. To prevent this you will just need to keep repositioning the head to face the other way. Try to position the infant's bouncy seat or car seat so that the child will want to face the way against the tilt of the head. This will cause the child to reposition its head naturally and learn to turn their head to both sides.
The most common concern with
Torticollis is a flat spot on the skull and abnormal face formations. Both of these can be easily prevented by exercise and repositioning. If your infant does develop a flat spot on its skull or face a helmet may be necessary to reform the skull. These helmets are fitted and checked weekly to assure they are working. The infant generally become very comfortable in the helmet, but they are expensive.
If you think your infant has
Torticollis schedule an appointment with your pediatrician soon. If your pediatrician confirms your worries you will be set up with a physical therapist to learn the proper techniques and stretches tailored to your son or daughter. You will probably have a check up every 2 weeks to see how your child is progressing.
Although Torticollis can be worrisome to any parent, it is highly treatable. If your infant seems to be uncomfortable or in pain a trip to the doctor is necessary! With a little bit of stretching and exercise your infant can have a straight neck once again!