Are flat heads in babies a sign of genius or a sign of the times? Centuries ago, the shape of a baby's head would indicate certain traits and talents, but today's parents often think their baby has something wrong with it if its head is not perfectly formed. And the fact is, flat-headed babies are on the rise. According to experts, the "back-to-sleep" movement that's been prominent worldwide in the past decade, a successful movement designed to protect babies from Sudden Infant Death Syndrome or SIDS, has resulted in an increased number of babies with flat heads.
That increase, coupled with our society's unfortunate focus on body image, has troubled some parents enough to send them to clinics that fit their flat-headed babies with helmets that have to be worn 23.5 hours a day; months of helmet-use encourages baby's head to grow into a socially desirable round shape.
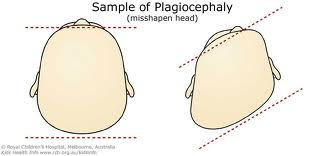
Flat-headedness even has a medical term -- plagiocephaly -- and until recently the condition was assumed to be of cosmetic concern only. But last month, results of a study of babies with the condition indicated that plagiocephaly might be a red flag for early neuro-devlopmental disadvantage, says researcher Dr. Matthew Speltz.
The clinical psychologist from the Seattle Children's Research Institute says that the so-called "disadvantage" he refers to is in the area of motor skills: In other words, up to one-quarter of the babies with flat-heads in his study were a little behind in their motor or movement skills compared to babies whose heads were not flat.
Speltz prefers the term positional plagiocephaly because the babies' flat heads are caused in part by their spending so much time on their backs ' sleeping in cribs, lying back in car seats and carriages.
"There's been a dramatic rise in positional plagiocephaly since the 1990s," he says. That coincides with the campaigns that urged parents to put their babies on their backs to sleep in order to protect them from SIDS.
In the 1970s, one in 300 infants had plagiocephaly, but by 2006 as many as one or two out of 10 babies had the condition.
"That increase, to all of us, is a small price to pay for the reduction in SIDS," says the pediatric researcher. "Many parents and doctors in the past dismissed it as a cosmetic issue, but our study suggests that we should look deeper."
Speltz and his team studied six-month old infants with and without flat heads, measured their skulls and assessed each using a respected scale of infant development. The flat-headed babies performed worse on their motor skills than the control subjects by an average of 10%.
"It's not that deformational or positional plagiocephaly causes neuro-developmental delay," explains Speltz. 'It's more that it's a marker of an elevated risk for delays."
Because babies who have flattened areas in the back of the head during the first year may be at risk for developmental delay, Speltz feels that pediatricians "should monitor closely the development of infants with this condition."
He says that it may be that flat-headed infants who show motor developmental delays will simply catch up with normal-headed babies by the time they're a year old and sitting up and moving more. (His team is in the process of examining that.)
"We need to look at their development down the road," he says.
"We don't want parents to think that flatness causes delay -- it's more an associated feature that may be a red flag. We want parents to continue to put babies to sleep on their backs. We hope that doctors will simply be more vigilant as to potential motor issues because early intervention is key and quite effective."
Baby helmet heads
The Clarren Helmet, used to treat uneven head shapes in babies, was invented at the Seattle Children's Hospital in 1979. The helmet, worn 23.5 hours daily from three to eight months in total, is designed so that the child's pliable head grows into the molded shape of the helmet. Pediatric researcher Dr. Mathew Speltz says that about 30% of parents whose babies have been diagnosed with plagiocephaly choose a helmet treatment for their babies. There are also other techniques used, including certain head bands.
Is your baby's head flat?
Remember that flat spots in a young baby's head can be common and by itself is no cause for alarm. Infants' skulls are soft and malleable until approximately one year. Other tips for parents and caregivers from the Seattle Children's Research Institute:
* If your baby is diagnosed with plagiocephaly, ask the doctor to screen for developmental delays in both motor and cognitive skills.
Talk about the results.
* Remember that babies develop at different times, and at different rates. What is 'normal' for your baby may be ahead of or behind what is normal for another baby. Babies who start out slower often catch up later.
* Always place babies to sleep on their backs: this remains the safest way to sleep. Place your baby's head at one end of the crib and switch to the other end the next night.
* Encourage active 'tummy time' when babies are awake: find ways to for baby to engage, play and move while on their tummy, several times each day. Watch your baby during tummy time.
* Choose different positions and ways for babies to play and be held: variety of stimulation is important. Switch the arm you use to cradle your baby each feeding session; right one time, left the next.
* Use strollers, car seats, infant seats, bassinets, cribs and play pens when necessary, but remember that babies need frequent lap time, cuddling, active play times and chances to move that aren't limited to being in stationary positions.
* Develop motor skills: play with babies to get them moving. Encourage crawling, rolling, reaching, pushing, pulling, holding, grasping.
* Develop cognitive skills: play with babies to get them thinking and talking. Encourage interactions with their environment, looking, listening, imitating, babbling, singing, talking, reading.
Source: chealth.canoe.ca | Marilyn Linton