A few words, from our peditrician, could have helped us and many other families to avoid plagiocephaly. One of the key words, that was left out of our early visits, is
repositioning.
What is "
repositioning"?
"Techniques to encourage your child to alter the resting position of his/her head."
Why is "
repositioning" important?
"Careful attention to repositioning while your child is awake can prevent or reduce positional cranial deformities."
From the American Academy of Pediatrics:
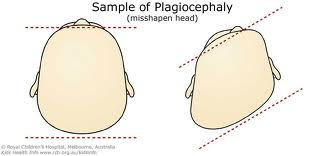
"To prevent the [deformational plagiocephaly], parents should be counseled during the newborn period (by 2 to 4 weeks of age) when the skull is maximally deformable. Parents should be instructed to lay the infant down to sleep in the supine position, alternating positions (i.e., left and right occiputs). When awake and being observed, the infant should spend time in the prone position. The infant should spend minimal time in car seats (when not a passenger in a vehicle) or other seating that maintains supine positioning....
Once deformational plagiocephaly is diagnosed, parents should be made aware of the condition and the mechanical adjustments that can be instituted. In general, most infants improve if the appropriate measures are conducted for a 2- to 3-month period. These include
positioning the infant so that the rounded side of the head is placed dependent against the mattress.
Additionally, the position of the crib in the room may be changed to require the child to look away from the flattened side to see the parents and others in his or her room..."
Source: Persing J, James H, Swanson J, Kattwinkel J. Prevention and management of positional skull deformities in infants. American Academy of Pediatrics Committee on Practice and Ambulatory Medicine, Section on Plastic Surgery and Section on Neurological Surgery. Pediatrics 2003 Jul;112(1 Pt 1):199-202.
Key points:
Infants should always be placed on their backs to sleep.
However to avoid positional plagiocephaly:
change the child's
sleeping position by placing the child's head at opposite ends of the crib on alternate nights
turn the crib around every few days -- babies will turn their head away from the wall
change the position of toys (for mobiles) and other objects to encourage head movement.
Include supervised "
tummy time" in your child's day. In addition to removing pressure on the back/side of the head, playing on his/her tummy is good for development.
Alternate the arm in which the infant is held for bottle and/or breast feeding.
During diaper changes, alternate the side from which you approach the infants. This will encourage the child to turn his/her head to look at the caregiver.